

For decades, academic literature has operated under a profound diagnostic paradox: it classifies Attention-Deficit/Hyperactivity Disorder (ADHD) strictly as a static attention deficit. Yet, clinical practice and frontline observation repeatedly witness the opposite—periods of intense, all-consuming concentration known as hyperfocus.
Because modern neuroscience has historically treated hyperfocus as an unquantifiable quirk rather than a primary mechanism of attention dysregulation, academic research remains shockingly sparse. This institutional negligence does not simply leave a gap in textbooks; it directly compromises the validity of diagnostic testing, driving a severe misdiagnosis of working memory impairments in ADHD individuals.
The Core Concept: A Clash of Metrics
When a brain capable of hyperfocus meets standard cognitive testing, the metrics shatter. Working memory—the brain's mental sticky note used to hold and manipulate short-term data—is traditionally measured via rigid, linear, and low-stimulus tasks (such as digit span or spatial tracking tests).
The academic negligence of hyperfocus distorts these measurements in two distinct directions:
1. The Masking Effect (The False Positive)
Standard neuropsychological assessments assume that a subject’s focus remains relatively stable during a testing session. However, the sheer novelty or high-stakes environment of a clinical evaluation can act as a massive dopamine trigger for an ADHD brain.
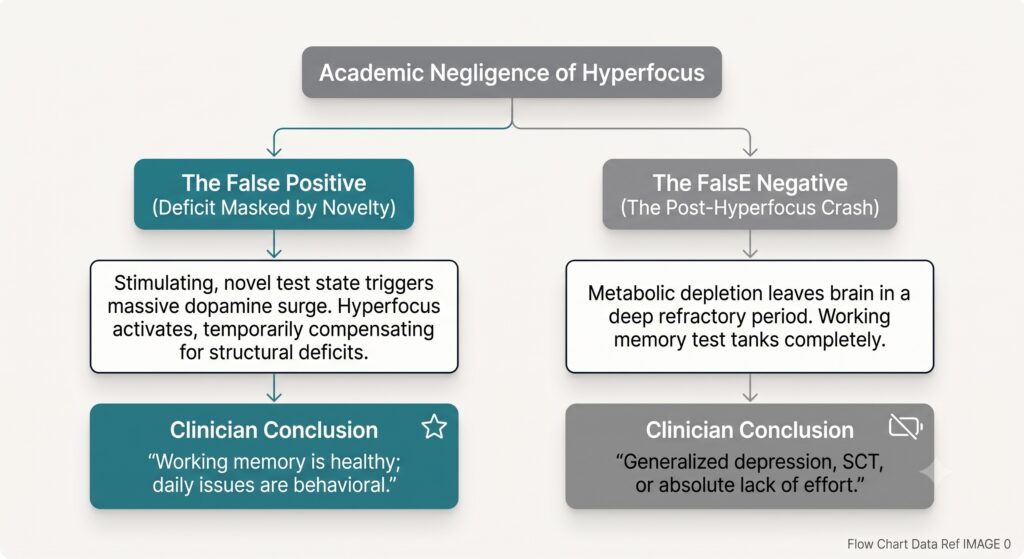
If the testing environment accidentally sparks a hyperfocused state, the individual can temporarily marshal tremendous cognitive resources. They track the numbers, hold the spatial coordinates, and achieve a high score.
Without academic frameworks that mandate long-term, dynamic, or contextual testing, clinicians interpret this peak performance as baseline health. The conclusion is almost always the same: "Their working memory functions fine when they want it to, so their daily struggles must be a behavioral choice or a lack of effort." In reality, an involuntary, transient state of hyperfocus masked a profound everyday structural impairment.
2. The Post-Hyperfocus Crash (The False Negative)
Hyperfocus is an incredibly expensive neurological state. It requires intense metabolic synchronization, burning through finite reserves of glucose and dopamine.
When an ADHD individual emerges from a prolonged hyperfocus episode—whether from an athletic competition, a coding sprint, or a creative project—the brain enters a severe, protective refractory state. During this "crash," the central executive network is starved, causing working memory efficiency to drop precipitously.
Because researchers have neglected to study hyperfocus longitudinally, clinicians rarely account for these cyclical fluctuations. If an individual is evaluated during a post-hyperfocus crash, their working memory performance will tank entirely. Without the context of the preceding hyperfocus state, this acute exhaustion is frequently misdiagnosed as Sluggish Cognitive Tempo (SCT), Major Depressive Disorder, or a generalized learning disability rather than a dynamic executive regulation issue.
The Silo Problem: Where the Real Experts Live
The ultimate irony of this research gap is that a group of clinicians already possesses a profound, working knowledge of hyperfocus mechanics: sports psychologists.
While mainstream clinical academia plays it safe inside sterile, static testing rooms, sports psychologists operate in high-octane, chaotic, real-world arenas. They are paid to optimize performance and manage energy regulation, forcing them to treat attention not as a static trait on a checklist, but as a dynamic, non-linear energy system.
| The Traditional Neuropsychologist | The Sports Psychologist |
| The Goal: Diagnose a static baseline deficit to justify accommodation or medication. | The Goal: Optimize high-octane performance and manage real-world energy regulation. |
| The Environment: A sterile, silent, low-stimulus office with a computer screen. | The Environment: High-stakes, high-stimulus, unpredictable athletic environments. |
| View on Hyperfocus: An unmeasured, problematic anomaly that disrupts linear focus. | View on Hyperfocus: A high-performance "zone" that requires deliberate aiming and recovery. |
Sports psychologists don't have the luxury of pretending the post-hyperfocus crash doesn't exist. In athletics, if a performer burns through their metabolic resources in a massive burst of hyper-synchronized focus, the drop-off in execution, real-time working memory, and situational awareness is immediate and visible on the field. They actively build training and recovery regimens around this exact refractory period.
Because they watch the human engine run at max RPM, sports psychologists routinely witness the ultimate working memory paradox: an athlete who can read an entire complex defense in a split second might completely forget where they put their car keys twenty minutes after the game ends.
The Structural Toll of Masking
Left without a proper diagnosis, many ADHDers learn to artificially induce hyperfocus through panic, anxiety, or high adrenaline just to force their unreliable working memory to hold a project's moving pieces together. Over time, relying on this extreme survival mechanism to bypass a working memory deficit leads to catastrophic executive burnout.
Moving Beyond the Deficit Paradigm
Until academic institutions align their research with real-world observations and bridge the gap with sports science, diagnostic testing will continue to fail. Hyperfocus and working memory deficits are not unrelated anomalies; they are two sides of the exact same fluctuating cognitive coin. Science must stop playing it safe with sterile lab environments and begin building dynamic, longitudinal metrics that measure the ADHD brain in its natural states of both flow and exhaustion.
For a deeper dive into how the academic gap surrounding hyperfocus leaves clinicians confused by these erratic shifts in attention, check out this video breakdown by ADHD & Hyper-Focus - Part I. This commentary explores the scarce scientific literature on hyperfocus, how it overlaps with flow states, and why the clinical world continues to struggle to establish it as a recognized feature of ADHD.