

For decades, mainstream ADHD discourse—spearheaded by figures like Dr. Russell Barkley—has relied heavily on a deficit-based, biologically deterministic model. This framework frequently points to structural neuroimaging studies revealing a 3% to 10% reduction in prefrontal cortex (PFC) volume or gray matter density in individuals diagnosed with ADHD.
The narrative built around this data is simple, clean, and highly marketable: ADHD is a congenital, genetic "hardware glitch." The PFC is structurally deficient; therefore, the individual cannot self-regulate.
However, this biological determinism is built on a fundamental misinterpretation of what "density" actually means, completely ignoring activity-dependent neuroplasticity. When we look at the rising tide of executive function (EF) deficits in supposedly "neurotypical" teenagers, alongside what the psychopharmacological data actually says about stimulants, the "congenital defect" argument begins to crumble under its own weight.
1. The Category Error of "Density Deficits"
An MRI scanner is a magnificent tool, but it does not measure "dysfunction." It measures physical proxies.
When a structural MRI detects a "density deficit" in the prefrontal cortex, it is not showing a lack of genetically pre-programmed brain cells. Instead, it is capturing a thinner neuropil—the dense, tangled web of dendritic branches, glial support cells, and synaptic connections.
These synaptic networks do not grow from a rigid, unyielding blueprint; they are activity-dependent. They are built, stabilized, and multiplied through rich, high-fidelity, three-dimensional physical feedback loops with the environment.
To blame a density deficit solely on a genetic "malfunction" while ignoring the child's environment is a complete reversal of cause and effect. It is the equivalent of looking at the atrophied leg muscles of an individual who has been forced to sit in a chair for a year, and declaring they suffer from a "congenital walking deficit."
2. The Great Convergence: "Neurotypicals" and EF Deficits
If a density deficit in the prefrontal cortex were a highly specific, congenital "marker" of ADHD, we would expect the structural and behavioral profiles of neurotypical teenagers to remain entirely distinct.
But that is not what is happening. We are currently living through a massive, uncontrolled experiment where "neurotypical" high schoolers are exhibiting unprecedented deficits in executive functioning: working memory decay, an inability to self-regulate, near-zero impulse control, and an incapacity for deep, sustained focus.
At the exact same time, large-scale neuroimaging initiatives—like the NIH’s Adolescent Brain Cognitive Development (ABCD) study tracking over 11,000 children—have found that heavy screen use (which replaces physical, tactile, and spatial experiences with flat, two-dimensional, passive stimulation) is associated with premature cortical thinning in the prefrontal cortex.
A Comparison of Experiential Environments
| Environmental Input (The "PFC Gym") | Modern Screen-Saturated Input (The "PFC Blindfold") |
| High physical feedback loops (spatial tracking, tactile coordination, physical trial-and-error). | Low physical feedback (flat glass screens, passive video consumption, virtual spaces with zero sensory depth). |
| Productive boredom, which forces the default mode network (DMN) to self-generate thought, planning, and internal reflection. | Constant external stimulation that instantly hijacks attention, starving the DMN and preventing internal executive control from developing. |
| Gradual dopamine rewards built on long-term effort and physical mastery. | Hyper-frequent, frictionless dopamine drops (short-form video algorithms, push notifications) that rewrite reward pathways. |
When you deprive any developing brain—whether labeled ADHD or neurotypical—of the three-dimensional, high-feedback environment it evolved to require, the prefrontal cortex cannot build its roads. The visual cortex of a kitten stitched blindfolded during development will wither and show a structural "deficit".
If we "blindfold" a teenager's prefrontal cortex from rich physical and cognitive experiences, we get the exact same result: a structural density deficit on an MRI.
3. The Structural Equivalence Paradox: The Threat to Barkley’s Argument
This brings us to a devastating logical paradox for the biological determinist model.
Imagine a series of neuroimaging studies that compare three groups of adolescents:
- Teens diagnosed with ADHD.
- "Neurotypical" teens with heavy screen/passive-sensory lifestyles who are exhibiting severe EF deficits.
- "Neurotypical" teens with highly active, tactile, low-screen lifestyles.
If the MRIs show that Group 1 and Group 2 have equivalent prefrontal density deficits compared to Group 3, what happens to Dr. Russell Barkley's argument?
It collapses.
The Deconstruction of the "Congenital ADHD" Narrative
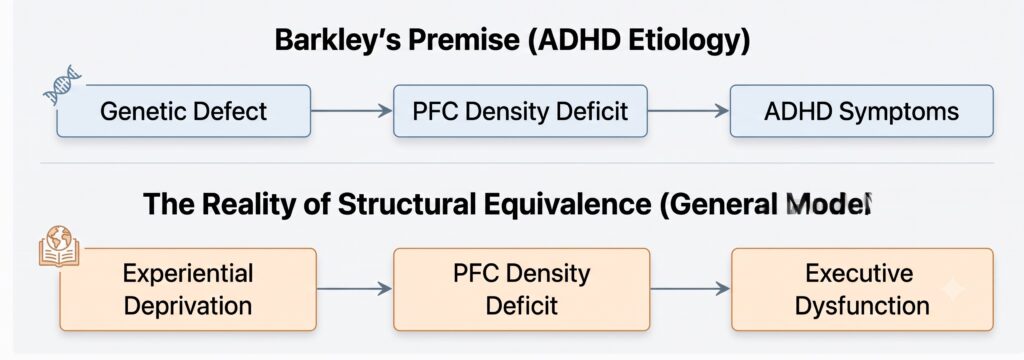
If a "neurotypical" teenager can acquire the exact same structural density deficit and executive dysfunction through experiential deprivation (screentime, sedentary lifestyles, passive learning), then a density deficit is not a diagnostic marker of an inborn ADHD pathology.
Instead, it is a universal biological response to a starved environment. You can no longer claim ADHD is a distinct, congenital "broken thermostat" when you can build the exact same "broken thermostat" in a healthy brain simply by changing its experiential inputs.
4. The Stimulant Proof: A Chimera of Cognitive Enhancement
To salvage the biomedical model, proponents often point to the dramatic effect of stimulants: "If stimulants fix the focus, it must be a neurochemical deficit!"
But this is where the psychopharmacological literature delivers the final blow. Extensive, double-blind, placebo-controlled studies have consistently shown that stimulants do not provide actual cognitive enhancement to neurotypicals.
- No Actual Cognitive Gains: When neurotypicals take stimulants (like Adderall or Ritalin), they do not show improvements in working memory, complex problem-solving, cognitive flexibility, or high-level executive functioning.
- The Productivity Illusion: In computationally complex tasks (such as the "knapsack problem" simulating real-world allocation of resources), neurotypicals given stimulants actually show a decrease in productivity and accuracy, taking 50% longer to solve problems because the flood of dopamine leads to "erratic thinking" and hyper-focus on irrelevant details.
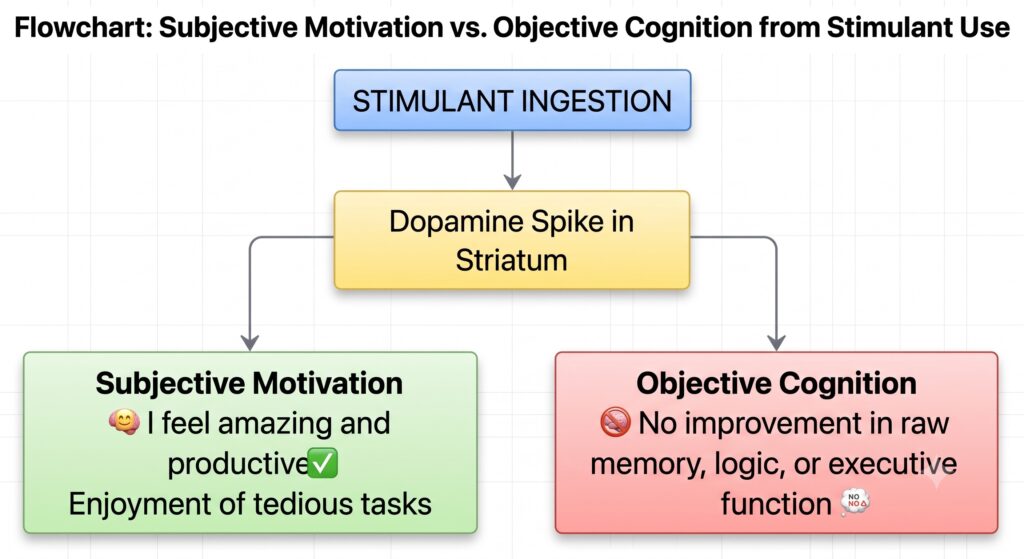
- The Motivational Trick: What stimulants actually do is increase task-enjoyment and subjective energy. They make a tedious, boring task feel highly interesting because they artificially spike dopamine in the striatum.
The brain on stimulants isn't "smarter" or "repaired"; it is simply highly motivated.
If stimulants do not objectively "fix" executive functioning in brains with acquired density deficits—and instead merely act as motivational grease—then treating them as a targeted "correction" for a specific congenital genetic defect is a profound category error.
Conclusion: Reclaiming the Environment
When we frame ADHD as a static, congenital brain defect, we let the modern, sedentary, hyper-stimulated environment off the hook. We treat the child as the problem, rather than looking at the sterile, two-dimensional cage we have placed them in.
A density deficit in the prefrontal cortex is not a life sentence written in our DNA. It is a physical testament to how desperately the human brain needs to interact, move, build, and play in the real, tactile world to grow its own roads. If we want to fix the "deficits" in our children's brains, we must first stop blindfolding them to the experiences that make us human.
For a deeper dive into how our modern environment actively shapes young brains, this report on how screen time alters child brain development highlights the structural changes researchers are seeing in real-time.