
⚠️ Crucial Clinical Disclaimer
The following material discusses complex neurobiological interactions, trauma frameworks, and emerging pharmacological research. This article is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.
ADHD and Complex PTSD (C-PTSD) share massive symptomatic overlap; self-diagnosing either condition—or assuming specific trauma pathways—can lead to inappropriate interventions. Furthermore, the use of mycelial hallucinogenics or empathogens (such as psilocybin and MDMA) carries significant psychological and legal risks, and should never be attempted outside of legally sanctioned, medically supervised clinical environments. Always consult a qualified physician or mental health professional regarding your health or the health of a child.
When a child with Attention-Deficit/Hyperactivity Disorder (ADHD) grows up in a highly volatile home, the line between genetic neurodivergence and developmental trauma begins to blur. Because ADHD is highly heritable—with roughly 74% of its variance tied to genetics—an ADHD child frequently has at least one ADHD parent.
When that parent is undiagnosed, untreated, and carrying their own unresolved childhood wounds, a devastating generational loop is born. The intersection of executive dysfunction, hypervigilance, and emotional dysregulation creates a profound, bi-directional overlap in the human nervous system—one that echoes from early childhood, through the turbulent high school years, and straight into adulthood.
1. The Domestic Trigger: A Collision of Dysregulated Nervous Systems
A child with ADHD naturally exhibits behaviors driven by an under-stimulated prefrontal cortex: impulsivity, emotional volatility, and difficulty following multi-step demands. In a household where the caregiver is an undiagnosed ADHD adult with unresolved trauma, the parent’s "window of tolerance" is inherently narrow.
Lacking the internal executive "brakes" to pause under stress, the parent frequently misinterprets the child's neurological roadblocks as intentional defiance or disrespect. Under high stress, the parent’s survival brain defaults to their own childhood conditioning, often resulting in harsh physical punishment or emotional abuse.
Statistical data underscores this vulnerability: individuals diagnosed with ADHD are roughly seven times more likely to report experiencing physical abuse during childhood than neurotypical peers. The child’s ADHD triggers the parent’s trauma, and the parent’s aggressive response inflicts new trauma back onto the child.
2. The High School Pivot: When Hyperactivity Turns to Rage
As these children enter high school, the presentation of their ADHD undergoes a profound shift. The outward, physical hyperactivity of childhood typically internalizes, transforming into chronic restlessness, anxiety, and deep emotional dysregulation.
When you layer a decade of childhood trauma onto this shift, the high schooler’s brain adopts a state of permanent hypervigilance.
- The Symbiotic Overlap: Developmental trauma alters the prefrontal cortex and hyper-activates the amygdala (the brain's threat center). Because a traumatized brain is constantly scanning for danger, normal school stressors—like being called out by a teacher or failing an assignment—are interpreted by the subconscious not as simple mistakes, but as imminent threats to safety.
- The Explosive Output: Lacking the top-down executive functioning controls to inhibit their reactions, these students experience rapid, intense outbursts of anger. To an outside educator, it looks like a simple anger management issue or Oppositional Defiant Disorder (ODD). In reality, it is a delayed manifestation of an overloaded nervous system using a "fight" response as a shield against deep-seated shame.
3. The Front Lines: School Interventions and Parental Sabotage
Traditional school discipline—such as suspension or zero-tolerance policies—acts as a validation of the student's trauma, reinforcing the belief that the world is inherently hostile and punitive. To break this, high school leadership teams must pivot to unified, trauma-informed strategies:
- Principals must shift from punitive measures to regulate-first policies, ensuring a student is physically de-escalated before processing a behavioral infraction.
- Counselors must provide proactive executive functioning anchors and discreet de-escalation passes to prevent crises before they boil over.
- Social Workers must utilize body-based somatic grounding and co-regulation—using their own calm presence to reset the student’s mirrored nervous system.
However, these interventions frequently collide with a systemic roadblock: parental sabotage. As a high schooler builds trust with a school social worker and begins to disclose the realities of an abusive home, the parent often panics. Driven by shame or fear of child welfare interventions, parents will abruptly pull the teenager out of mental health care, weaponizing logistical or financial excuses.
To counter this, school teams increasingly rely on federal education laws like the Individuals with Disabilities Education Act (IDEA). By legally embedding social work and counseling services directly into a student's binding Individualized Education Program (IEP) or 504 Plan, the mental health care is transformed from an optional medical treatment into a protected educational right that a parent cannot unilaterally cancel.
4. The Architecture of Healing: Dissolving the Compartments
For adults or older adolescents attempting to heal from this dual engine of ADHD and trauma, traditional talk therapy often fails because it requires a fully functional prefrontal cortex—the exact region taken offline by stress. Furthermore, the brain frequently copes with early childhood terror by creating amnesic walls, completely compartmentalizing the trauma into hidden pockets of the subconscious.
To access these forgotten layers, clinical research has turned to emerging bottom-up treatments, specifically highlighting the stark neurobiological differences between compounds like MDMA and mycelial hallucinogenics like psilocybin.
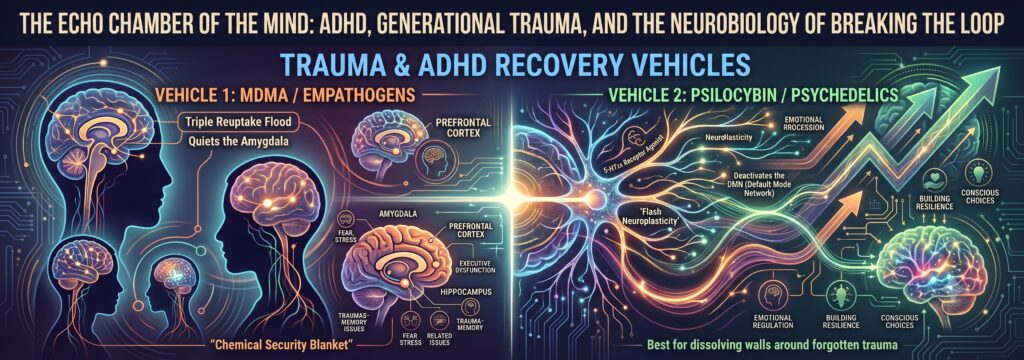
While MDMA acts as a chemical security blanket—quieting the amygdala and flooding the brain with oxytocin so a person can tolerate looking at known, horrific memories—psilocybin acts as a dissolver of cognitive structures.
Psilocybin targets the Default Mode Network (DMN), the brain's rigid traffic cop responsible for maintaining defensive ego barriers and keeping compartmentalized memories isolated. By temporarily deactivating the DMN, psilocybin allows isolated neural networks to communicate, bringing forgotten visual, emotional, and somatic memories safely to the surface without triggering the standard survival panic.
Capturing the Window of "Flash Neuroplasticity"
This process triggers what can be described as flash neuroplasticity. By flooding the brain with Brain-Derived Neurotrophic Factor (BDNF), the substance stimulates rapid dendritic spinogenesis—the physical budding of new neural connections. Simultaneously, it softens the perineuronal nets, the structural scaffolding that locks adult memory circuits in place.
This creates a highly malleable, temporary "open critical period" lasting roughly one to two weeks post-treatment. During this integration runway, the individual can look at the newly unearthed childhood memory through a safe, adult lens. As the brain naturally cools down and the perineuronal nets harden once again, the memory is re-consolidated. It is no longer locked away as a volatile, hidden landmine driving unexplained adult rage, but is finally integrated as a normal, peaceful piece of personal history.
By physically restructuring how the brain stores its oldest defenses, this neuroplastic window offers the rare opportunity to permanently sever the generational chain of trauma.